Заглавная страница Избранные статьи Случайная статья Познавательные статьи Новые добавления Обратная связь FAQ Написать работу КАТЕГОРИИ: ТОП 10 на сайте Приготовление дезинфицирующих растворов различной концентрацииТехника нижней прямой подачи мяча. Франко-прусская война (причины и последствия) Организация работы процедурного кабинета Смысловое и механическое запоминание, их место и роль в усвоении знаний Коммуникативные барьеры и пути их преодоления Обработка изделий медицинского назначения многократного применения Образцы текста публицистического стиля Четыре типа изменения баланса Задачи с ответами для Всероссийской олимпиады по праву 
Мы поможем в написании ваших работ! ЗНАЕТЕ ЛИ ВЫ?
Влияние общества на человека
Приготовление дезинфицирующих растворов различной концентрации Практические работы по географии для 6 класса Организация работы процедурного кабинета Изменения в неживой природе осенью Уборка процедурного кабинета Сольфеджио. Все правила по сольфеджио Балочные системы. Определение реакций опор и моментов защемления |
Coulthard MG, Lambert HJ, Keir MJ.Содержание книги
Поиск на нашем сайте
Occurrence of renal scars in children after their first referral for urinary tract infection. BMJ1997; 315: 918-919. Downs SM. Technical report: urinary tract infections in febrile infants and young children. The Urinary Tract Subcommittee of the American Academy of Pediatrics Committee on Quality Improvement. Pediatrics 1999; 103: e54. Hansson S, Martinell J, Stokland E, Jodal U. The natural history of bacteriuria in childhood. Infect Dis Clin North Am 1997; 11: 499-512. 8. Hellerstein S. Urinary tract infections. Old and new concepts. Pediatr Clin North Am 1995; 42: 1433-1457. Nuutinen M, Uhari M, Murphy MF, Hey K. Clinical guidelines and hospital discharges of children with acute urinary tract infections. Pediatr Nephrol 1999; 13: 45-49. Rosenfeld DL, Fleischer M, Yudd A, Makowsky T. Current recommendations for children with urinary tract infections. Clin Pediatr Phila 1995; 34: 261-264. RushtonHG. Urinary tract infections in children. Epidemiology, evaluation, and management. Pediatr Clin North Am 1997; 44: 1133-1169. Shalaby-Rana E, Lowe LH, Blask AN, Majd M. Imaging in pediatric urology. Pediatr Clin North Am 1997; 44: 1065-1089. Shapiro E, Elder JS. The office management of recurrent urinary tract infection and vesicoureteral reflux in children. Urol Clin North Am 1998; 25: 725-734. 14. Smellie JM, Rigden SP. Pitfalls in the investigation of children with urinary tract infection. Arch Dis Child 1995; 72: 251-255. Stapleton A, Stamm WE. Prevention of urinary tract infection. Infect Dis Clin North Am 1997; 11: 719-733. Stark H. Urinary tract infections in girls: the cost-effectiveness of currently recommended investigative routines. Pediatr Nephrol 1997; 11: 174-177. Weidner W, Ringert R-H, Rascher W. Leitlinie zur Harnwegsinfektion im Kindesalter. Urologe A 1998; 37: 669-770. 18. Weiss RA. Update on childhood urinary tract infections and reflux. Semin Nephrol 1998; 18: 264-269. 19. Williams MA, Noe HN, Smith RA. The importance of urinary tract infection in the evaluation of the incontinent child. JUroM994; 151:188-190.
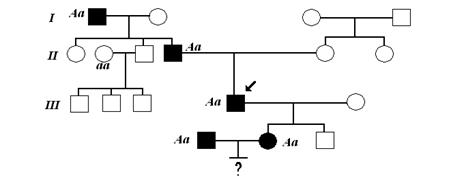
BACKGROUND VUR or VRR are defined as non-physiological back-flow of urine from the urinary bladder into the ureter or the renal pelvis. The worst consequence of both primary and secondary VRR is the development of progressive renal failure secondary to recurrent pyelonephritic episodes and subsequent loss of renal parenchyma. Ten to 15% of patients with reflux suffer from a renin-dependent hypertension as a sequela of focal ischaemia due to parenchymal scarring. The probability of hypertension is highly correlated with the extent and number of parenchymal scars. Reflux is found in 0.5-1 % of normal children without UTIs. While in newborns the incidence of reflux is the same in both sexes, in later life, girls are approximately four times more frequently affected than boys. In children with recurrent UTI, the incidence of VUR is significantly higher (about 14-29% of kindergarten and school girls and about 30% of boys of the corresponding age). The main symptoms of VUR are recurrent and occasionally febrile UTIs. Radiological investigations verify uni- or bilateral reflux in 30-50% of cases. A VRR may also make itself apparent in later stages by its consequences, such as hypertension, renal insufficiency or delayed renal growth. Undetected reflux may lead to reflux nephropathy. Secondary reflux Predecessor of a secondary reflux is not an inborn primary disturbance of the terminal ureter, but rather an anatomically or functionally obstructive or inflammatory illness of the bladder, or direct damage to a previously intact orifice. It seems that many refluxes, especially of lower grade l-lll, are secondary refluxes and may disappear with the maturation of the bladder function. CLASSIFICATION The International Reflux Study Committee introduced a uniform system for the description of reflux, based on the earlier classification by Heikel and Parkkulainen, in 1985. Furthermore, a standardized performance of a voiding cystourethrogram was described to allow comparative studies.
|
||||
|
|
Последнее изменение этой страницы: 2017-01-19; просмотров: 204; Нарушение авторского права страницы; Мы поможем в написании вашей работы! infopedia.su Все материалы представленные на сайте исключительно с целью ознакомления читателями и не преследуют коммерческих целей или нарушение авторских прав. Обратная связь - 3.147.81.172 (0.006 с.) |

 7. REFLUX
7. REFLUX