Заглавная страница Избранные статьи Случайная статья Познавательные статьи Новые добавления Обратная связь КАТЕГОРИИ: ТОП 10 на сайте Приготовление дезинфицирующих растворов различной концентрацииТехника нижней прямой подачи мяча. Франко-прусская война (причины и последствия) Организация работы процедурного кабинета Смысловое и механическое запоминание, их место и роль в усвоении знаний Коммуникативные барьеры и пути их преодоления Обработка изделий медицинского назначения многократного применения Образцы текста публицистического стиля Четыре типа изменения баланса Задачи с ответами для Всероссийской олимпиады по праву 
Мы поможем в написании ваших работ! ЗНАЕТЕ ЛИ ВЫ?
Влияние общества на человека
Приготовление дезинфицирующих растворов различной концентрации Практические работы по географии для 6 класса Организация работы процедурного кабинета Изменения в неживой природе осенью Уборка процедурного кабинета Сольфеджио. Все правила по сольфеджио Балочные системы. Определение реакций опор и моментов защемления |
Involvement of the brain and cranial nerves
1.Comminution of the ethmoid occurs with Le Fort II and III fractures and some severe fractures of the nasal complex. This may lead to a dural tear in the region of the cribriform plate of the ethmoid resulting in cerebrospinal rhinorrhoea (Fig. 4). A dural tear may also occur adjacent to fractures involving the posterior wall of the frontal sinus. Cerebrospinal fluid may also escape into the soft tissues via coincident fractures of the orbital roof without appearing in the nasal cavity. More rarely, a profuse cerebrospinal fluid rhinorrhoea occurs as a result of a fracture which passes through the base of the sphenoid, communicating with the sphenoidal sinus and via a crack in the roof of this structure with the middle cranial fossa. 2. Damage to the infra-orbital and zygomatic nerves may occur with zygomatic and Le Fort II fractures either unilaterally or bilaterally. This gives rise to anaesthesia or paraesthesia of the skin of the cheek and upper lip. Full recovery of sensation may be delayed for up to two years. The anterior, middle and posterior superior alveolar nerves are frequently damaged leading to anaesthesia of the upper teeth and gingiva. 3. Cranial nerves within the orbit may sustain damage in zygomatic, Le Fort II and III fractures. The sixth cranial nerve is most frequently involved but sometimes the contents of the superior orbital fissure are all damaged, in which case ophthalmoplegia, dilation of the pupil and anaesthesia within the distribution of the ophthalmic branch of the fifth cranial nerve are severally noted. Rarely the orbital apex is fractured with resultant damage to the optic nerve and blindness.
Figure 1. Anatomical specimen showing the disarticulated bones of the skull exploded and mounted to demonstrate their complex interrelationship. Note that the bones of the mid-facial skeleton are all comparatively fragile. They comprise, from above downwards, the ethmoid, flanked by the two lacrimal bones. Next are the paired nasal bones, palatine bones, maxillae and inferior conchae with the zygomatic bone laterally on each side. The vomer is missing. Courtesy of the Anatomical Museum, Royal College of Surgeons of England.
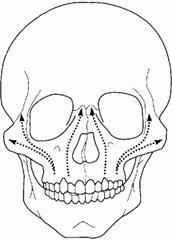
Figure 2. Diagram showing the directions of distribution of the forces of mastication within the skeleton of the mid-face.
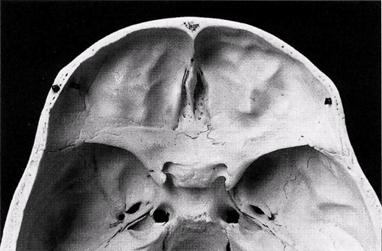
Figure 3. Diagrammatic representation of the strength of the bones of the skull and face. The 'matchbox' structure of the mid-facial skeleton cushions the effect of impact force B. Impact force A is transmitted directly to the brain producing the most severe injury. Impact force C is transmitted indirectly to the cranial base via the rigid structure of the mandible (represented here as a bent baseball. 4. Figure 4. The cribriform plate of the ethmoid. This fragile bone is fractured in Le Fort II and III type fractures and also in severe injuries of the naso-ethmoidal complex. Involvement of the orbit 1. The globe of the eye and the optic nerve are remarkably well protected by the physical structure and arrangement of the bones of the orbit. The prominence of the zygomatic bone acts as a protection for the globe from all impinging objects other than very small projectiles. The optic foramen is a ring of compact bone and in high level or Le Fort III injuries, fractures almost invariably pass around it. Rupture of the globe or tearing of the optic nerve is fortunately therefore rarely found with other than the most severe middle third fractures. 2. Fractures involving the orbit may give rise to alteration in the position of the globe of the eye. The level of the globe is normally maintained by the suspensory ligament of Lockwood, which passes from its medial attachment on the lacrimal bone to be inserted laterally into Whitnall's tubercle situated on the inner aspect of the zygomatic bone just below the frontozygomatic suture. Zygomatic and Le Fort III fractures commonly result in separation at this suture line with a resulting drop in the level of the globe of the eye.
3. If the bone comprising the floor of the orbit is fractured, orbital contents may herniated through into the maxillary sinus below. The resulting entrapment of these tissues may result in restriction of movement of the inferior rectus and inferior oblique muscles although, anatomically, the muscles themselves are not actually ensnared by fragments of bone. Alternatively, the muscles may become bound down adjacent to the damaged bone by subsequent fibrous tissue formation. In either event, temporary or permanent diplopia results due to prevention of the upward and outward rotation of the eye. The lateral rectus muscle may be partially paralysed by haematoma formation or sixth nerve neuropraxia adjacent to a fracture line resulting in lateral diplopia. Diplopia results mainly from interference with the activity of the ocular muscles rather than physical displacement of the globe. Extreme displacement of the latter will, however, result in such distortion of the visual axis that the muscles will be unable to compensate and double vision will be inevitable. 4. Orbital contents may also herniate through the thin lamina papyracea of the ethmoid bone on the medial wall of the orbit. Any significant increase in the orbital volume occurring as a result of fracture of the walls of the orbit will lead to enophthalmos. Enophthalmos, particularly if accompanied by inferior displacement of the lateral canthal attachment, may give rise to pseudo-ptosis, a physical sign traditionally referred to as 'hooding of the eye'. 5. Le Fort II and III fractures and severe nasal complex injuries may involve the naso-lacrimal duct with resulting epiphora. This complication is not noticed at the time of injury, but may become apparent later. 6. Detachment of the medial canthal attachment of the eye may occur in severe naso-ethmoidal injuries, giving rise to traumatic telecanthus. 7. Haemorrhage within the orbit is a frequent occurrence in facial injuries. In the absence of actual damage to the globe of the eye it is not usually significant. However, haemorrhage within the muscle cone of the eye (retrobulbar haemorrhage) can very rarely lead to loss of vision. Ord (1981) conducted a comprehensive review of this complication. It is now thought that blindness occurs as a result of spasm of the short posterior ciliary arteries, causing ischaemia of the optic nerve head over a limited but critical area. The paranasal sinuses In zygomatic complex and Le Fort I, II and III fractures, the maxillary sinuses are involved. The thin bony walls of the sinuses are often grossly comminuted with bleeding into the cavity and not infrequently inward herniation of the buccal pad of fat. This results in one or more of these paranasal sinuses appearing opaque on radiological examination. Apart from the routine reduction and repositioning of the fracture, no other special treatment is required and the radiological appearance of the sinuses will clear after about 6 weeks. Kreidler and Koch (1975) carried out an endo-scopic study of the maxillary sinus after mid-facial fractures in 25 patients and found 35 per cent had chronic mucosal changes, but all were free of symptoms. No similar studies appear to have been carried out to confirm these observations. Uncommonly, air may escape into the soft tissues of the face following a fracture which extends into one or other paranasal air sinus. This usually affects the flaccid tissues of the eyelids and leads to 'surgical emphysema'. This in turn gives rise to the physical sign of 'crepitation' of the soft tissues when palpated. Whenever air gains entry into soft tissue planes it is contaminated and adds to the risk of subsequent infection. Air within the cranial cavity and meninges or in the mediastinum is particularly dangerous and can rarely occur as a complication of facial trauma.
Important blood vessels The third part of the maxillary artery and its terminal branches are closely associated with the lines of fracture in Le Fort I, II and III - type injuries. Occasionally the artery or its greater palatine branch is torn in the region of the pterygomaxillary fissure or pterygopalatine canal resulting in severe life-threatening haemorrhage into the nasopharynx. Packing of the nose via the anterior nares, whilst usually sufficing in more minor nasal haemorrhage, will be ineffectual in this event. A post-nasal pack must be inserted, which will apply direct pressure to the bleeding point without embarrassing the airway through the mouth. It is necessary to retain this pack for 24 hours and to replace it if necessary. Such a pack is a potent source of infection and is not well tolerated by the patient. Adequate reduction of the fracture will fortunately prevent further bleeding in most cases. Multiple fractures The same association of direct with indirect violence may give rise to multiple fractures. The most common multiple fracture is that caused by a fall on the mid-point of the chin resulting in fractures of the symphysis and both condyles. These fractures are commonly seen in epileptics, elderly patients who lose consciousness as a result of general disease, and occasionally in soldiers who faint on parade, from which the fracture combination derives its name of 'guardsman's fracture'. Oikarinen and Malmstrom (1969), in a series of 600 mandibular fractures, found 49.1 per cent were single, 39.9 per cent had two fractures, 9.4 per cent had three fractures, 1.2 per cent had four fractures and 0.4 per cent had more than four fractures. Comminuted fractures Comminution of a fracture site is almost invariably the result of considerable direct violence at the site of fracture, as is commonly the case in war missile injuries (Fig. 5). In civilian practice this degree of comminution is most common in the symphysis and parasymphyseal regions. Such fractures require special management and should therefore be considered in a category of their own. It is not unknown for severe missile injuries to cause comminution of the whole of the mandible from one condylar neck to the other.
Figure 5. Lateral oblique radiograph showing comminuted fracture of the left body of the mandible following a medium-velocity missile injury
|
||||||
|
|
Последнее изменение этой страницы: 2021-01-08; просмотров: 83; Нарушение авторского права страницы; Мы поможем в написании вашей работы! infopedia.su Все материалы представленные на сайте исключительно с целью ознакомления читателями и не преследуют коммерческих целей или нарушение авторских прав. Обратная связь - 52.15.59.163 (0.007 с.) |