Заглавная страница Избранные статьи Случайная статья Познавательные статьи Новые добавления Обратная связь FAQ Написать работу КАТЕГОРИИ: ТОП 10 на сайте Приготовление дезинфицирующих растворов различной концентрацииТехника нижней прямой подачи мяча. Франко-прусская война (причины и последствия) Организация работы процедурного кабинета Смысловое и механическое запоминание, их место и роль в усвоении знаний Коммуникативные барьеры и пути их преодоления Обработка изделий медицинского назначения многократного применения Образцы текста публицистического стиля Четыре типа изменения баланса Задачи с ответами для Всероссийской олимпиады по праву 
Мы поможем в написании ваших работ! ЗНАЕТЕ ЛИ ВЫ?
Влияние общества на человека
Приготовление дезинфицирующих растворов различной концентрации Практические работы по географии для 6 класса Организация работы процедурного кабинета Изменения в неживой природе осенью Уборка процедурного кабинета Сольфеджио. Все правила по сольфеджио Балочные системы. Определение реакций опор и моментов защемления |
Allergic manifestations in childrenСодержание книги Поиск на нашем сайте
Within recent years numerous apparently diverse conditions such as asthma, hayfever, eczema, urticaria, migraine and other minor affections have been shown to have a similar etiologic basis, a hypersensitivity on the part of the sufferer to many usually harmless articles commonly encountered in his diet or environment. To this group of diseases the term ‘allergic’ has been applied; the individuals manifesting such an exaggerated susceptibility to substances innocuous to normal persons in the amounts commonly encountered are said to be ‘allergic’ to those articles; and the agents giving rise to those reactions in such apparently minute doses are termed ‘allergens’. When we analyse the origin of these allergic responses we find that they arise in one of two ways: either as a definite inheritance of a predisposition to manifest specific hypersensitiveness, or acquired as the result of tissue damage or excessive irritation. Though the allergic tendency is prenatal in origin the actual manifestations and causative allergens generally depend upon postnatal factors. The site and type of reaction are frequently consequent upon some local strain or injury, and selectivity of the allergen generally follows repeated or continuous contact with some factor of diet or environment. Allergic diseases have several characteristics in common the determination of which proves of the utmost importance in diagnosis. They are essentially periodic in nature with apparent intervals of freedom. The symptoms frequently have their onset at night or are most distressing during those hours. With the exception of hayfever the different manifestations have their maximum onset during childhood or adolescence, and each manifestation appears to have definite sex and seasonal variations. In addition, allergic conditions are definitely affected by varied states of health of the sufferer, by intercurrent diseases, such as fever, exanthemata or climatological factors, locality, altitude or environment. Varied manifestations of disease in childhood have been shown to fall into the allergic category. The commoner of these include such respiratory symptoms as recurrent bronchitis and asthma; such cutaneous eruption as eczema, flexural pruritis, urticaria including the popular and giant types, and purpura; such abdominal conditions as food-upsets, colic and recurrent vomiting, hayfever, migraine, enuresis and reactions to therapeutic serums and physical agents Much can be done to prevent the development of allergic symptoms in children, especially children of allergic parents. The homes should be as free from dust and allergens as possible. New foods should be tried one at a time, at least a week apart, to see if symptoms occur. Asthmatic children should be guided away from dusty occupations. Exposure to colds should be minimized. Psychosomatic factors, if present, should be given proper attention.
HEMOPHILIA
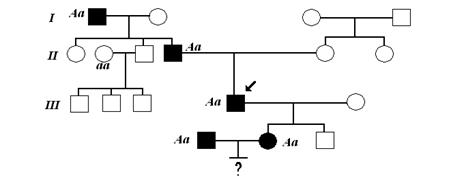
The hemophilias are a group of inherited disorders characterized by decreased clotting factor activity, with prolonged and often spontaneous bleeding. Hemophilia A, or classic hemophilia, is by far the most common form of disease and results from subnormal factor VIII activity. Until recently it was thought that factor VIII was absent., but it is now recognized that material identified antigenically as factor VIII is present, although procoagulant activity is reduced. It is currently believed that factor VIII has two components. Measuring each component independently permits detection of carriers, as well as a clear delineation from von Willebrand’s disease. In the latter, procoagulant activity is present disproportionate to the amount of protein antigen, and platelet abnormalities are present as well. Hemophilia B (Christmas disease) results from deficient factor IX activity. Both hemophilias A and B are sex-linked disorders; however, the mutation rate for hemophilia A is said to be upward of 25%, one of the highest known in human disease, von Willebrand’s disease is autosomally transmitted and thus affects both sexes equally. For reasons that remain unclear, hemophilia is rarely manifested on the first day of life, even after a difficult delivery. Factor VIII does not cross the placenta, yet the newborn with hemophilia does not experience increased bruising or unusually severe cephalhematomas. Even after circumcision, 75% of affected neonates have only mild or no bleeding; a complication from the procedure implies severe disease, defined as less than 1% normal activity. The first few months of life are usually a benign period during which the only clinical clues to the diagnosis may be exaggerated bruising from contact with crib slats. When walking – and falling – begins, excessive bruising and bleeding, particularly of the lip and tongue, are noted. Ecchymoses and soft-tissue bleeding remain common in childhood.
B. Тексты для устного и письменного тестирования.
AIDS PATIENT GIVEN BABOON BONE MARROW San Francisco. A pioneering experiment involving the first-ever transplantation of bone marrow into a human being is proceeding well, according to researchers from the University of California at San Francisco and the University of Pittsburgh. Last week, J.Getty, a 38-year-old AIDS patient, received baboon bone marrow, in the hope that a mixture of baboon and human marrow could help to reconstitute his damaged immune system. Baboons are not susceptible to HIV, and, if experiment is successful, the chimaeric bone marrow will begin producing immune system cells resistant to the virus. Several days after the transplant, Getty was reported to be doing well. But doctors said he would remain vulnerable to neutropenia – a decrease in the number of neutrophilic leukocytes in the blood – and opportunistic infections for several weeks. Researchers should be able to measure how well the baboon cells have taken in about four weeks, but doubt they will see any immune reconstitution in under six months. The protocol for the experiment had been given strict scrutiny by federal authorities, partly because of concern that the introduction of baboon cells into a human might trigger the development of new viruses. S.Ildstad, a researcher involved in the experiment, said that monitoring for such organisms has already begun, with samples being collected weekly for examination by collaborators throughout the world. Formal guidelines for xenotransplantation are being developed by the Food and Drug Administration and the Centres for Disease Control. Ildstad praised Getty’s brevity and said many patients might ultimately benefit.
ALCOHOL’S YOUNGEST VICTIMS
Drinking during pregnancy is riskier than many women realize.
Everyone in the US should know by now that drinking alcohol during pregnancy can cause serious physical and mental problems in the unborn child. Most doctors have told their patients, television announcements have dramatized the danger, and warning signs have gone up in restaurants and bars. But too many mothers-to-be are not getting the message. More than 50,000 babies are born in the US each year with alcohol-related defects. In about one-fourth of these cases, the damage – ranging from facial deformities to heart abnormalities – is severe enough to be classified as fetal alcohol syndrome. Many people still do not realize how common FAS is and how devastating it can be. According to some researchers, FAS is responsible for an estimated 20% of all US cases of mental retardation. That makes FAS the country’s No.1 threat to children’s mental health, greater than either Down syndrome or spina bifida. Unlike such drugs as barbiturates and opiates, which affect the nervous system, alcohol can attack virtually any of the body’s cells. It can cause stunted growth, distorted faces, poor eyesight, learning disabilities and hyperactivity. In the recently published book “The Broken Code”, the author Michael Dorris tells the heartbreaking story of his adopted son Adam, whose Sioux parents dies of alcohol abuse. Adam was institutionalized and diagnosed as retarded before he turned three. At five, he still wore diapers, could not count consecutively or even identify color. “Adam’s birthdays are reminders for me,” writes Dorris. “For each celebration commemorating that he was born, there is the pang, the rage, that he was not born whole”. The tragedy of FAS is that it is entirely preventable. If a woman, even an alcoholic one, stops drinking before she tries to become pregnant, her fetus will not develop FAS or any alcohol-related birth defects. But pregnancies are not always planned. If a woman does not realize for several weeks that she is pregnant, she may not stop drinking in time to prevent harm to the fetus. Researchers believe the damage is probably minimal in the first two weeks, but during the rest of the first trimester, when the fetus’ organs are forming, the effects may be especially severe. If the drinking continues, additional damage can occur, since the brain develops during all nine months and rapid body growth does not occur until the third trimester. Even after the baby is born, abstinence may be advisable. A study in “New England Journal of Medicine” suggests that when mothers have one or more drinks a day, their children ingest alcohol in breast milk, which may impede the infant’s motor development. Nearly all known cases of FAS involve children whose mothers have chronic alcohol problems. The more a woman drinks while she is pregnant and the longer she drinks, the higher the risk of FAS. Even so, moderate drinking is not considered safe. But our best evidence is that we cannot detect adverse consequences to very light drinking. And that does not mean they don’t exist. Beer, wine and hard liquor do not seem to differ in their impact on the fetus. Studies conducted in Boston, Atlanta and Scandinavia indicate that at least some of the injuries to the fetus may be corrected in the womb if a mother gives up alcohol before her third trimester. It’s pretty clear if a woman stops drinking in her second trimester, the size and the healthiness of the baby will improve, but there is no evidence that its intelligence will improve. Moreover, even the improvement in appearance may be deceptive. The babies definitely are bigger and look healthier but that does not mean that all the effects go away. Scientists still do not know why FAS strikes the children of some alcoholic mothers but not others, and why susceptibility varies among different ethnic groups. Native Americans, for example, are 33 times as likely as Caucasians to have a child with FAS; for blacks, the rate is 6.7 times as high as for Caucasians. Women who give birth to a child with FAS have a greater-than-average risk of bearing additional children with the affliction. Such evidence suggests there may be a genetic predisposition to FAS, but scientists have not been able to identify the offending genes. Researchers are also trying to determine whether fathers’ drinking habits play any role in FAS. At Wayne State, studies of male laboratory rodents have shown that alcohol exposure affects their sperm as well as the immune system and behaviour of their offspring. The possibility of the father’s effect can not be written off. Researchers are not saying the baby would have FAS, but it’s possible there may be some impact on how the kid comes out. There is no treatment for FAS, and so the only way health officials can fight the scourge is to step up educational efforts. The couple must read a pamphlet on FAS before they can obtain a marriage licence / in New Hampshire/. Beginning in November, liquor bottles will carry a warning label advising women that alcohol and pregnancy do not mix. But for women who are addicted to alcohol, the need to drink often overcomes caution and reason. Until better ways are found to identify and treat alcoholics, they will continue to inflict a devastating toll on their children.
VITA MEANS LIFE
For centuries, scurvy was a real scourge among seamen and explorers, and no one knew how to combat it. Rickets, which afflicted small children, pellagra, beriberi and other diseases also remained an enigma. In 1881, Nikolai Lunin, a Russian physician, put forward the hypothesis of the existence of some substances that are essential for life. These substances were isolated in their pure form more than 30 years later by K.Funk, a Polish researcher, who called them vitamins - “carriers of life”. Today we know some 30 vitamins and vitamin-like substances. Scurvy, rickets, beriberi and pellagra have been established to be all avitaminoses, i.e., diseases caused by the lack or deficiency of one vitamin or another in the organism. Nowadays doctors come across avitaminoses comparatively rarely. Other problems connected with vitamins attract much more attention. Our scientists are of the opinion that nucleic acids play the main part in the process of growth and propagation of cells. They proved that vitamin C (ascorbic acid) regulates one of the stages in the formation of desoxyribonucleic acid – the famous DNA. Vitamin K, one of the “youngest” vitamins, discovered only some 30 years ago, is of great importance for the proper coagulation of blood. It is essential for the formation of prothrombin, a proteic substance necessary for clotting a blood vessel to stop a hemorrhage. In 1942, Academician Al.Palladin, a prominent Russian biochemist, and his staff synthesized vikasol, a new preparation, which contains an analogue of vitamin K. During World War II, vikasol won a good repute for itself among army doctors. Injected intramuscularly or intravenously, it quickly stops various hemorrhages. Now it is used as a preparation against inflammation and as a means for increasing the resistance of organisms to radioactive irradiation. But vitamin K is essential not only for blood clotting. It plays an active role in the so-called tissue breathing of the organism’s cells, in the metabolism. It is as necessary for each living cell as air is vital for man. The doctors use vitamins on a wide scale of treatment – with the aid of vitamins they influence the metabolism in the direction they want, and increase the resistance of the organism to various diseases. For instance, orotic acid, a substance which possesses vitamin-like properties, and which is a factor for growth, is used to intensify the contracting function of the myocardium, when the latter has been disrupted by prolonged stress. The preparation Kalium orotium is used to treat such a grave and dangerous disease as a large-focal infarct of the myocardium (heart failure). The use of this preparation (in combination with folic acid and vitamin B12) at the clinic made it possible to decrease the number of deaths from this disease. Apart from this, the patients’ blood pressure improves and they recover much more quickly and are even able to go back to their usual work. Good results have been obtained by administrating Kalium orotium to patients with other cardio-vascular disorders. The researchers think, that this preparation will possibly be used to treat ulcers of the stomach and duodenum, to speed up the healing of wounds and burns and also other diseases and traumas, when the organism needs an accelerated synthesis of protein.
Active words and expressions.
Scurvy, beriberi, pellagra, deficiency, avitaminosis, to inject, to play an active role, inflammation, to obtain, wound, burn, to improve, to accelerate, resistance.
VITAMINS
Vitamins are dietary substances required by the body in very small amounts for normal biochemical function. There are two major groups: water-soluble vitamins (the B vitamins and vitamin C), and the fat-soluble vitamins A, D, E and K. Intensive research into their sources, their function and our requirements for them has been going on over the last sixty years or so and we now know a great deal about them. Vitamin A. The term vitamin A covers several fat-soluble compounds including retinal, which is the most important component, and two lesser components, retinal and retinoic acid. Vitamin A is only found in animal produce but various vitamin-A-type compounds, the most important of which is beta-carotene, are found in vegetables, and these are water-soluble. All of them are fat-soluble, are sensitive to light and are easily oxidized. Though the deficiency signs of vitamin A were recognized in ancient Egyptian times, it was only in the century that its chemical nature was elucidated. Two researchers recognized a substance described as “fat-soluble A” as being a growth-promoting factor in animals. Later it was shown that vitamin A activity was present in plants in the yellow pigments known as carotenes. What it does. The most important and well-known role of vitamin A is in relation to eye function. Vitamin A is necessary to prevent drying of the eye (xerophthalmia) and corneal changes; also, the normal function of the retina, the part of the eye involved with vision, and particularly the function of the light-sensitive areas of the eye, are dependent upon there being sufficient vitamin A. Vitamin A is involved in a number of other bodily functions. It is important in maintaining the stability of cell membranes and this may be clinically important. Furthermore, beta-carotene is the most effective receptor of free radical oxygen and this may be relevant in situations involving cancer, inflammatory disease and atherosclerosis, in which free radical mechanisms are thought to play a part. A connection between vitamin A and zinc metabolism has been described by several researchers. It appears that in severe zinc deficiency the formation of the protein which carries vitamin A, retinolbinding protein, is described. Zinc is an important constituent of many enzymes, including one found in the retina that is involved in vitamin A metabolism. Night blindness which does not improve with vitamin A supplements has been described in zinc deficient individuals, particularly in alcoholics with liver disease who are often vitamin A and zinc deficient. In diseases such as alcoholic cirrhosis, pancreatic disease and cystic fibrosis, zinc and vitamin A and other deficiencies also often occur together. Food sources: The major dietory sources are from animal produce, which provides vitamin A-retinol – usually combined with a fatty acid. As vitamin A is stored in animal and fish livers, these provide the most concentrated sources. Others include kidneys, eggs, milk and butter. Margarine is, by law, fortified with vitamin A. Good vegetable sources include any green, yellow or orange-pigmented produce; the darker the colour, the higher the content of beta-carotine. Carrots, spinach, cabbage and orange and yellow fruits are the best sources. Deficiency symptoms and signs. Vitamin A deficiency, one of the commonest and most serious world-wide nutritional deficiencies, occurs in people who have malabsorption states. In particular, anyone with fatty stools caused by pancreatic disease, biliary obstruction, or small bowel disease, is at risk. The earliest symptoms of vitamin A deficiency include night blindness (difficulty in seeing well in dim light) and dryness of the eyes. Skin signs of vitamin A deficiency include follicular hyperkeratosis, a condition in which the whole hair follicle and its adjacent skin is raised by a plug of horny keratin. Dryness of the skin can be a feature of vitamin A deficiency but this may be due to an associate essential fatty acid deficiency or a deficiency of other micronutrients such as vitamin B complex. Vitamin C and zinc are involved in fatty acid metabolism. Deficiency can occur without skin signs. In general vitamin A deficiency is associated with poor growth and development, and impaired resistance to infection.
HEMOCHROMATOSIS?
S. Foster’s health began to collapse in 1990, during her second pregnancy. “It was like somebody hit me over the head with a sledge hammer.” She had no energy. Her joints ached. She walked like a drunk woman. Some days she was so tired she couldn’t move from the couch. She would sit in her husband’s lap and cry and tell him, “Just put me in a home when I can’t go any more.” Foster visited a dozen doctors and investigated every explanation she could think of: Mercury poisoning? Copper poisoning? Multiple sclerosis? No one could tell her what was wrong with her. It wasn’t until 1995 that she got an answer: hemochromatosis. Hemochromatosis is an inherited blood disorder that causes the body to store excess iron. A normal person’s body absorbs the iron that it needs and lets the rest pass through. But people with hemachromatosis have no shut-off mechanism. Their bodies absorb and absorb, storing the extra iron in the joints, liver, heart and pancreas. This can cause arthritis, cirrhosis of the liver, diabetes, heart problems – and eventually, death. Hemochromatosis is the most common genetic disorder in the US. More than a million Americans have hemochromatosis, and another 10% carry one gene for the disorder. “It’s much more common than people realize,” said Dr. R.Brodkin, a Winston-Salem hematologist. The good news is that treatment is simple. Patients can control iron levels simply by giving blood. How often patients need to give depends on how much iron they have absorbed. Foster gave 36 pints of blood in 39 weeks. “After giving the blood, almost immediately, I felt a little bit lighter,” she said. But losing that much blood took its toll. At times, she felt more exhausted than she had before. But a few months after she finished the intense bloodletting, her health returned. “I feel much better. I still have joint pain. That will be lifelong.” But, she said, “I feel like a suit of armor has been lifted off my body.” She now gives a pint of blood three or four times a year. Foster, 38, is a nurse at High Point Regional Hospital. But in all of her years of nursing she never heard the word hemochromatosis until her mother, who suffers from liver disease, visited a new doctor who tested her blood and told her that she had the disorder. After Foster read about it, she was sure that she had it too. Blood tests and a liver biopsy confirmed her suspicions. More tests revealed that an aunt, an uncle and both of her sisters have hemochromatosis as well. She believes that her father, who died a number of years ago of a massive heart attack, also had it. Throughout her experience, Foster has been frustrated by many doctors’ lack of knowledge or interest in hemochromatosis. “The ignorance is just rampant in the medical community.”
Dr.G.Block agrees. He is a graduate of Bowman Gray School of Medicine and the medical director of the Hemochromatosis Center at the University of Pittsburgh Medical Center Health System. Studies have shown that it takes patients with full-blown hemochromatosis an average of 3 ½ to 5 years and seven to 11 doctors to get a diagnosis, he said. And until about a year ago, professors devoted maybe five minutes of medical school time to hemochromatosis and told students that the disorder was extremely rare. A new genetic test is raising the disorder’s profile. Before the development of the test, doctors couldn’t identify hemochromatosis until it had already caused a lot of damage. And determining whether hemochromatosis or something else was causing the problem required a liver biopsy, a relatively painful and involved procedure. Now the genetic test provides a quicker, easier answer. The test isn’t perfect. It identifies only 85% of people with hemochromatosis, Block said. The other 15% of people with the disorder got it through some other gene problem doctors can’t identify yet. One reason that doctors didn’t catch the disorder earlier, Brodkin and Block said, is because most insurance companies don’t cover the routine iron-level screenings that would indicate a problem. The tests aren’t that expensive, usually between $60 to $120. And studies show that the average undiagnosed hemochromatosis patient racks up $20,000 a year in medical bills, according to David Snyder. Snyder is the executive director and vice president of the American Hemochromatosis Society. The society is educational and advocacy group that is pushing blood banks to accept hemochromatosis patients’ blood. Right now patients must go to a doctor and pay to have blood drawn. “There’s nothing wrong with the blood,” Brodkin said. “It would be very safe for this blood to be used for transfusions, but the Red Cross won’t accept it.” It is also pushing for genetic testing for all newborns. He said that currently, only about 3% of all people with hemochromatosis know that they have the disorder. People who are carriers need to know that, too, he said. Carriers can have somewhat elevated iron levels, Brodkin said. And being a carrier can worsen certain existing problems, such as liver disease or heart trouble. Also, if two carriers marry, they have a 25% chance of passing the disease on to their children. The need-to-know is what has Foster out talking to anyone who asks about hemochromatosis. “One of the reasons I do this is because I know there’s another Shiryl out there, who thinks she’s lost her mind, who thinks she’s just a whiner.”
ANEMIA
Anemia, one of the more common disorders, occurs when the number of healthy red blood cells decreases in the body. The disc-shaped red blood cells contain hemoglobin, a unique molecule that carries oxygen to the body’s tissues. Anemia occurs for different reasons. These include: 1. increased destruction (break down) of red blood cells (RBCs); 2. increased blood loss from the body; 3. inadequate production of red blood cells by the bone marrow. In some cases anemia results from an inherited disorder, whereas in other cases the condition is caused by something in a person’s environment, such as a nutritional problem, infection, or exposure to a drug or toxin. Signs and symptoms of the disease: The most common sign of iron deficiency and other types of nutritional anemia is mild paleness of the skin, along with decreased pinkness of the lips, the lining of the eyelids, and the nail beds. A friend or relative who sees your child only occasionally may be more likely to notice this than you because the changes usually happen so gradually. Other common signs of anemia may include: irritability, fatigue, dizziness, lightheadedness, and a rapid heartbeat. Depending on the condition causing the anemia, other signs and symptoms may occur, such as jaundice (yellow-tinged skin), dark tea-colored urine, easy bruising or bleeding, and enlargement of the spleen or liver. In infants and preschool children, iron-deficiency anemia can result in development delays and behavioral disturbances, such as decreased motor activity and problems with social interaction and attention to tasks. Recent research studies indicate that behavioral problems may persist into and beyond school age if the iron deficiency is not properly treated. Diagnosing anemia: In many cases doctors don’t discover anemia until they run blood tests as part of a routine physical examination. A complete blood (CBC) may indicate that there are fewer red blood cells than normal. Caring for a child with anemia: the type, cause and severity of the child’s anemia will determine what kind of care she needs. In general, though if your child has significant anemia, she may tire more easily than other children and therefore need to limit her activity. Make sure that her teachers and other caregivers are aware of her condition. If iron deficiency is the cause, follow her doctor’s directions about dietary changes and iron supplementation. If the spleen is enlarged, your child may be prohibited from playing contact sports because of the risk of rupture and hemorrhage. Treatment for anemia depends on the cause of the condition. It’s important not to assume that any symptoms your child may be having are due to iron deficiency. Be sure to have her checked by a doctor, and don’t attempt to treat her yourself before doing so. If a certain medication appears to be the cause, your child’s doctor may discontinue it or replace it with something else – unless the benefit of the drug outweighs this side effect. If an infection is the cause, the anemia will usually get better when the infection passes on its own or it is cured by treatment. Treatment for more severe or chronic forms of anemia may include (depending on the cause): 1. transfusions of normal red blood cells taken from a donor; 2. removal of the spleen or treatment with medications to prevent blood cells from being removed from the circulation or destroyed too rapidly; 3. medications to fight infection or stimulate the bone marrow to make more blood cells. Whether anemia can be prevented depends on the cause of the condition. Presently there is no way to prevent anemia that is caused by genetic defects affecting the production of red blood cell or hemoglobin. However there are steps you can take to help prevent iron deficiency – the most common form of anemia. Before following any of these suggestions, be sure to talk them over with your child’s doctor.
|
||||
|
|
Последнее изменение этой страницы: 2016-08-16; просмотров: 430; Нарушение авторского права страницы; Мы поможем в написании вашей работы! infopedia.su Все материалы представленные на сайте исключительно с целью ознакомления читателями и не преследуют коммерческих целей или нарушение авторских прав. Обратная связь - 216.73.216.220 (0.009 с.) |