Заглавная страница Избранные статьи Случайная статья Познавательные статьи Новые добавления Обратная связь КАТЕГОРИИ: ТОП 10 на сайте Приготовление дезинфицирующих растворов различной концентрацииТехника нижней прямой подачи мяча. Франко-прусская война (причины и последствия) Организация работы процедурного кабинета Смысловое и механическое запоминание, их место и роль в усвоении знаний Коммуникативные барьеры и пути их преодоления Обработка изделий медицинского назначения многократного применения Образцы текста публицистического стиля Четыре типа изменения баланса Задачи с ответами для Всероссийской олимпиады по праву 
Мы поможем в написании ваших работ! ЗНАЕТЕ ЛИ ВЫ?
Влияние общества на человека
Приготовление дезинфицирующих растворов различной концентрации Практические работы по географии для 6 класса Организация работы процедурного кабинета Изменения в неживой природе осенью Уборка процедурного кабинета Сольфеджио. Все правила по сольфеджио Балочные системы. Определение реакций опор и моментов защемления |
Numerous epidemiologic time-series studies have shown generally consistent associations of outdoor (ambient) air pollution with cardiovascular hospital admissions.Стр 1 из 4Следующая ⇒
Outdoor Air Pollution
Rural areas Rural areas are affected by outdoor air pollution primarily from burning agricultural land and forest fires. In addition, with growing desertification, dust storms may become major contributors to contaminants in the air.
Air pollutions are mostly emitted by local sources but some fraction of the pollution is also transported through the atmosphere from the sources located outside, sometimes in a far distance.
Urban settings Urban pollution comes from many sources, stationary (industrial emissions) and mobile (vehicles), as well as natural ones, such as soil erosion.
Urban air pollution is caused by a mixture of pollutants including: 1. sulfur oxides (SOx), 2. nitrogen oxides (NOx), 3. carbon monoxide (CO), 4. ozone (O3) 5. organic compounds (VOCs) such as benzene, toluene, xylene and benzo(a)pyrene 6. lead is a noteworthy air contaminant in countries where it is added to gasoline, 7. particulate matter (PM).
Several of pollutants are very toxic and/or carcinogenic.
These pollutants are further transformed by processes in the atmosphere. For example, ground level ozone is a secondary pollutant produced by the interaction of sunlight with nitrogen dioxide and volatile organic compounds. Temperature and humidity are also important.
Environmental particulate air pollution is measured using several measures: - TSP – the mass of total suspended particles; - PM10 - mass of particles with an aerodynamic diameter of 10 µm. This closely corresponds to the mass fraction of inhaled particles that penetrates beyond the larynx to the airways. - PM2,5 -mass of particles with an aerodynamic diameter of 2,5 µm. The respirable fraction, which penetrates to the unciliated regions of the lung.
Particles that are less than 100 nm in diameter are commonly defined as ultrafine. Ultrafine particles are found to a large extent in urban air as both singlet and aggregated particles. Ultrafine particles are very small compared with the cellular structures and so this may be important in the apparent problems they present to the lung. Particles of diesel exhaust may be taken as an example of an ultrafine particle. They are largely insoluble because of the particulate carbon core, commonly the size of singlet diesel particles is 10–20 nm. However, they tend to group into aggregates with sulphates, metals, and hydrocarbons.
In many cities, urban air pollution is magnified by heavily polluting industrial complexes, which, although initially located and built outside the city, following urban developments are now located within the city or close to its periphery. The stationary sources that contribute most to the volume of air pollution emissions are: 1. the energy and heat generation sector, 2. the mining industry, 3. the metals industry, and 4. the chemicals industry, including refineries. Among them, the biggest polluters are power generation stations.
At the same time, both the absolute and relative amounts of pollution emitted by mobile sources are becoming more important, as traffic increases and emissions from industry decreases.
For example, here in Russia the mobile sources are rapidly growing in number and so are their emissions. The vehicle fleet, both public and private, is ageing on average. It is still using poor quality motor fuels. Poor maintenance of old vehicles, the lack of effective traffic management and the decline of public transport in most urban areas complete the picture. As a result of down-sizing of stationary sources and drastic decrease in public transport volume the share of mobile sources in total national emissions of nitrogen oxides, VOCs and carbon monoxide has been systematically increasing. In some cities transport is responsible for up to 75% of total emission of selected pollutants, and is solely responsible for air toxins like benzo(a)pyrene and soot.
Health effects Health impacts of exposure to air pollutants present in urban atmosphere are well recognized. Studies conducted in many parts of the world in the recent decades have demonstrated a wide range of health effects associated with the pollution in concentrations commonly observed in the cities.
Mortality For Western countries, it is estimated that tens of thousand of premature deaths annually are associated with the pollution. Studies have found increased risk of cardiopulmonary and noncancer respiratory deaths with exposure to ambient particulate matter, ozone, and nitrogen oxides.
Morbidity PM and Health Several studies on short-term effects have found that ambient PM increases cardiac arrhythmia, decreases heart rate variability, increases the inflammatory response measured by C-reactive protein (CRP), and increases blood viscosity as well as other blood markers (e.g., hemoglobin, fibrinogen, platelet counts, white cell counts). These observed effects would provide a mechanism by which chronic exposure to ambient air pollution is associated with risk of coronary heart disease (CHD).
Estimated effects of air pollution on daily mortality APHEA2 and NMMAPS studies
The APHEA2 mortality study covered a population of more than 43 million living in 29 European cities, which were all studied for > 5 years in the early-mid 1990s.
The APHEA2 hospital admission study covered a population of 38 million living in 8 European cities, which where studied for 3 to 9 years in the early-mid 1990s.
The NMMAPS mortality study covered a population of more than 50 million living in 20 metropolitan areas in the United States of America, which were all studied over the 1987–1994 period.
The NMMAPS hospital admission study covered 10 large metropolitan areas in the United States of America with a combined population of 1 843 000 subjects over 65 years old.
Asthma Asthma is a chronic inflammatory disease with symptoms including reversible airway constriction, chest tightness, cough, and wheezing. The incidence of asthma is increasing. Asthma develops most commonly in children, although recent data suggest an increase in new cases among adults and the elderly. An individual’s risk for developing asthma is defined by a complex interaction of environmental exposures and hereditary factors. Risk factors include urbanization. Numerous epidemiological studies have linked air pollution to exacerbation of acute asthma, increased use of asthma medication, increased school and work absence, and increased hospitalization. Toxicological research has characterized several components of air pollution, including particulate matter (PM), gaseous elements such as ozone, microbial products including endotoxin, heavy metals, and indoor and outdoor allergens such as house dust mite allergen and ragweed.
Respiratory health Numerous studies have reported adverse effects of air pollution on the respiratory health of children, using indicators of general air pollution and of traffic-related air pollution. In Europe, studies have found that more than 10% of children ages 13-14 suffer from asthma, with a significant burden of disease attributable to outdoor air pollution. Some studies have investigated the expected beneficial effects of air pollution reduction on respiratory health in children. In cross-sectional analysis, the tremendous decline of coal combustion-related air pollution in East Germany after reunification was associated with a decline of respiratory symptoms and improved lung function in children. In a cohort of children, those who moved within California to areas with lower PM10 levels showed increased lung function growth, whereas those moving to more polluted areas had a decreased growth. A rather moderate decline of air pollution levels in the 1990s in Switzerland was associated with a reduction in respiratory symptoms and diseases in school children.
Blood lead levels In the last decade children’s blood lead levels have fallen significantly in a number of countries. Despite this reduction, childhood lead poisoning continues to be a major public health problem for certain at-risk groups of children, and concerns remain over the effects of lead on intellectual development in infants and children. The evidence for lowered cognitive ability in children exposed to lead has come largely from prospective epidemiologic studies. The main sources of lead in children’s environments are diet, lead-based paint in older housing, lead in soil and dust from contaminated leaded paint and gasoline, or past and present mining and industrial activity. Exposure from air and waterborne sources has been greatly reduced with the introduction of unleaded gasoline and the replacement of lead water pipes and water tanks with nonlead alternatives. However, lead in soil and dust continues to be a major source of exposure.
Three groups of reasons, which can explain children's vulnerability to air pollution, should be mentioned: 1. Behavioral reasons: Younger children are often unaware of health risks around them and are typically unable to make choices to reduce their risk. For example, hand to mouth behavior, typical of very young children, exposes them to lead dust and other harmful substances deposited from the air. 2. Physiological reasons: Children breathe more air than adults do in proportion to their body weight. Children also react to certain toxicants more severely than adults because of their narrower air passages and their smaller size. Given their small stature, children's breathing zones are closer to the ground which can expose children to high concentrations of air pollutants. 3. Developmental reasons: Children's lungs are growing rapidly during the first year of life and they continue to develop air sacs through their first four years. Exposure to air pollutants during these formative years could hinder normal lung development. The developing nervous system is thought to be far more vulnerable to the toxic effects of lead than the mature brain.
Pregnancy outcomes The study of birth outcomes is an important emerging field of environmental epidemiology. Birth outcomes are important in their own right because they are important indicators of the health of the newborns and infants. In addition, low birth weight (LBW), intrauterine growth retardation (IUGR), and impaired growth in the first years of life are known to influence the subsequent health status of individuals, including increased mortality and morbidity in childhood and an elevated risk of hypertension, coronary heart disease, and non-insulin-dependent diabetes in adulthood. I’d like to present you the review on the evidence linking adverse birth outcomes with ambient air pollution. The birth outcomes have been divided into five groups: a) mortality of fetuses and infants, b) LBW, c) premature (preterm) births, d) IUGR, and e) birth defects. The evidence is sufficient to infer a causal relationship between air pollution and respiratory deaths in the postneonatal period. The studies found an association between sulfur dioxide and total suspended particles and respiratory mortality in the postneonatal period. For air pollution and birth weight the evidence suggests causality, but further studies are needed to confirm an effect and its size and to clarify the most vulnerable period of pregnancy and the role of different pollutants (particular matters, sulfur dioxide, carbon monoxide, nitrogen oxides). For preterm births and intrauterine growth retardation (IUGR), as well as birth defects, the evidence as yet is insufficient to infer causality, but the available evidence justifies further studies. Molecular epidemiologic studies suggest possible biologic mechanisms for the effect of air pollution on birth weight, premature birth, and IUGR. It has been shown that the levels of DNA adducts are positively related to risk of IUGR, birth weight, birth length, and head circumference, and hypoxanthine-guanine phosphoribosyltransferase (HPRT) locus mutation frequency in infants. In terms of exposure to specific pollutants, particulates seem the most important for infant deaths, and the effect on IUGR seems linked to polycyclic aromatic hydrocarbons, but the existing evidence does not allow precise identification of the different pollutants or the timing of exposure that can result in adverse pregnancy outcomes. Ambient air pollution and pregnancy outcomes: a review of the literature by Radim J. Sram, Blanka Binkova, Jan Dejmek and Martin Bobak Environmental Health Perspectives April 2005 v113 i4 p375(8)
Air pollution control
Practically, all countries have adopted legislation /regulation. Policy objectives STANDARDS AND MEASUREMENTS RUSSIAN FEDERATION In Russian Federation air quality is evaluated in reference to the former Soviet Union reference values (the state standards). These include more than one thousand pollutants. The standards are called maximum allowable concentrations (MAC), and mainly consist of short-term (20 to 30 minutes) or daily average concentrations. Generally, MACs are stricter than WHO guidelines, except for some heavy metals or PM. Vehicles emissions are also subject to state standards, which have not been revised since Soviet times, and are less strict than any EU or UN/ECE or United States standards.
WHO AIR QUALITY GUIDELINE:
The most relevant instruments for compliance and enforcement of clean air policy objectives are (PRINTOUT16): 1. licensing polluting activities; 2. inspection; 3. economic instruments; 4. and monitoring activities. Policy instruments INSPECTION Compliance with the norms for stationary sources is controlled by the State Ecological Inspectorate, and is established in most of the NIS through instrumental measurements.
ECONOMIC INSTRUMENTS The available economic instruments in the NIS are emission charges and fines, established in general for pollutant classes, depending on their toxicity. Fines are applied when emissions exceed standards, or are several times higher. All money collected is channeled to the National Budget or to National or Regional Environmental Fund, where existing, from where it is then allocated for different environmental projects. Inspection of in-use vehicles should be systematic and inspectors and road police have to be well equipped for this task.
URBAN AIR MONITORING Problem solving should start with its analysis. Urban air monitoring is one the ways, and there are a lot of things have to be done. Let’s look at situation in Russia. 1. Data from urban monitoring are available for selected pollutants. 2. None of the data are very reliable. The main reason is low precision of the 20 minutes sampling. More reliable continuous or automated sampling is generally not yet available. 3. Also, urban air monitoring stations are not always properly sited so the monitoring results are inadequate to represent population exposure. 4. However, the most important weakness of any urban monitoring in Russia is the lack of capacity to fully monitor and analyze particulate matter, taking into account its size composition. HEALTH IMPACT ASSESSMENT It is still worth noting that health impact assessments have not yet been combined with licencing procedures in a single permit procedure. Health concerns should be part of the decision-making process for new investments and health authorities or professionals have to be involved in these decisions.
PUBLIC AWARENESS Public awareness should be rapidly raised. Only then will political attention focus on the issue, and direct the necessary resources to environmental health care.
INDOOR AIR POLLUTION Solid fuel Many people in industrialized nations give little thought to central heating, electric lighting, and flick-of-a-switch cooking. But more than half of the people in the world rely on solid fuels to heat and light their homes and cook their food.
This percentage varies widely between countries and regions, ranging from 77%, 74%, and 74% in Sub-Saharan Africa, Southeast Asia, and the Western Pacific Region, respectively, to 36% in the Eastern Mediterranean Region, 16% in Latin America and the Caribbean and in Central and Eastern Europe. In most industrialized countries, solid fuel use falls to the < 5% mark. Cooking and heating with solid fuels on open fires or traditional stoves in poorly ventilated indoor environments leads to high levels of indoor air pollution. Indoor air pollution comprises a variety of health-damaging pollutants including particles, carbon monoxide, nitrous oxides, sulfur oxides (mainly from coal), formaldehyde, and carcinogens, such as benzo[a]pyrene and benzene. Studies from Asia, Africa, and the Americas have shown that indoor air pollution levels are extremely high in households that rely on biomass fuel or coal: for example, 24-hr mean levels for PM10 in homes using biomass fuels range from 300 to 3,000 µg/m3. By comparison, the U.S. Environmental Protection Agency (EPA) annual air pollution standard for PM10 is 50 µg/m3 and WHO AQG – 20 µg/m3. Thus, typical concentrations of indoor air pollutants exceed many times the generally accepted guideline limits for outdoor air pollution. Indoor air pollution has been associated with a wide range of health outcomes, and the evidence for these associations was classified as strong, moderate. There is consistent evidence that exposure to indoor air pollution increases the risk of pneumonia and other acute lower respiratory infections (ALRIs) among children under 5 years of age, chronic obstructive pulmonary disease, and lung cancer (in relation to coal use) among adults above 30 years of age. Young children are often carried on their mother’s back during cooking or kept close to the warm hearth. Consequently, children spend many hours breathing indoor air pollution during their first year of life, when their developing airways and immature immune systems make them particularly vulnerable to hazardous pollutants. The evidence for a link with cancer, asthma, cataracts, and tuberculosis was considered moderate. Given limited available studies to date, there is tentative evidence for an association between indoor air pollution and adverse pregnancy outcomes, in particular low birth weight, ischaemic heart disease, interstitial lung disease, and nasopha-ryngeal and laryngeal cancers. Indoor air pollution was identified as the eighth most important risk factor and responsible for 2.7% of the global burden of disease. Globally, indoor air pollution from solid fuel use accounted for 1.6 million deaths and 39 million disability-adjusted life years (DALYs; a measure combining years of life lost due to disability and death) in the year 2000. In developing countries with high-mortality, indoor air pollution was responsible for 3.7% of the overall disease bur-den, making it the most important risk factor after malnutrition, unsafe sex, and lack of safe water and adequate sanitation.
Environmental tobacco smoke Environmental tobacco smoke (ETS) is also extremely dangerous to children's health. An estimated 700 million children worldwide breathe air polluted by tobacco smoke. Exposure to environmental tobacco smoke is associated with a range of harmful effects in children, such as respiratory tract infections, coughing and wheezing, worsening of asthma, and middle ear disease. Other suspected links include cardiovascular disease later in life, and possibly neuro-behavioral harm. Exposure of pregnant women to environmental tobacco smoke is associated with low birth weight. ETS is associated also with Sudden Infant Death Syndrome.
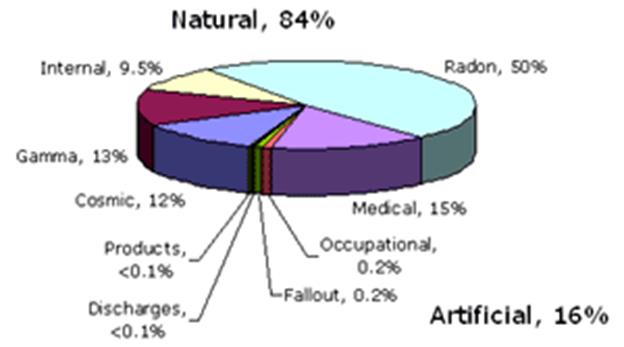
Radon
Radon is a natural radioactive gas which seeps into buildings from minute amounts of uranium that are present in all rocks, soils, brick and concrete. Radon levels in homes vary during the day, from one day to the next, and from winter to summer, mainly because of temperature differences between indoors and outdoors. They are generally higher at night and during the winter. Most people receive a larger radiation dose from radon indoors than from any other source, whether from the many industrial uses of radiation, nuclear power or medical exposures. There is a great deal of evidence that exposure to radon, or rather its decay products, leads to lung cancer in miners. Although the evidence from miners is clear, it is less easy to detect the effects of radon in houses because of the small number of people exposed at high radon levels in their homes, and the difficulty of measuring past exposures. Nevertheless, researchers are undertaking such studies. The most reliable are those that use individual data on radon exposures and smoking histories. Results from the largest domestic case-control study to date were recently published by researchers in Sweden. This study was based on 1360 lung cancer cases and roughly twice as many controls. The lung cancer risk was shown to increase to a statistically significant degree with increasing radon exposure and the risk estimates were consistent with those from the miner studies. The quantification of risk in studies of domestic exposure is, however, hampered by the lack of statistical power.
The contribution of environmental tobacco smoke and radon on the incidence of lung cancer has been estimated to be considerable. The source of formaldehyde, classed by IARC as a group 2A probable human carcinogen, in indoor air is mainly from furnishing materials and cigarette smoke. Levels indoors have been shown to be 10 times greater than levels outdoors.
(1) Regarding the causes of cancer: (a) tobacco is the most important preventable cause (b) occupational and environmental factors cause a high proportion of all cancers (c) geophysical factors are responsible for a large number of non-fatal cancer cases (d) all aspects of diet contribute to increased cancer rates (e) occupational exposures will continue to contribute a high proportion of future cancer incidence (2) Air pollution (a) air pollution has been associated with an increased risk of lung cancer (b) lung cancer rates in urban areas are higher than in rural areas (c) indoor air quality is not likely to contribute to cancer (d) environmental tobacco smoke causes lung cancer (e) air pollution definitely causes forms of cancer other than lung
(1) Which of the following is the correct defined size of ultrafine particles? (a) > 100 µm (b) < 100 nm (c) < 1000 µm (d) < 500 nm (e) < 10 nm (2) Are the following associated with increases in PM10? (a) Deaths from respiratory causes (b) Symptoms of fever (c) Worsening of symptoms of asthma in patients with pre-existing asthma (d) Deaths from heart attacks (e) Attacks of chronic obstructive pulmonary disease (COPD) (3) Which of the following is true of PM10 sampling convention measures? (a) Mass of particles with a 50% efficiency for those with an aerodynamic diameter of 50 µm (b) Mass of particles with 50% efficiency for those with an aerodynamic diameter of 10 nm (c) Mass of particles with 10% cut off for those with an aerodynamic diameter of 50 µm (d) Mass of particles with a 50% efficiency for those with an aerodynamic diameter of 10 µm (e) Number of particles with 50% efficiency for those with an aerodynamic diameter of 50 µm (4) Which of the following statements on ultrafine particles is not correct? (a) They are found in large numbers in urban air (b) They have a large surface area per unit mass (c) The form aggregates (d) They have a smaller surface area than the same mass of larger particles (e) They can exert their effects through mechanisms other than transition metals (5) Which of the following groups are susceptible to the adverse effects of PM10? (a) Patients with asthma (b) Patients with cystic fibrosis (c) Patients with COPD (d) Patients with cardiovascular disease (e) Patients with hayfever
Outdoor Air Pollution
Rural areas Rural areas are affected by outdoor air pollution primarily from burning agricultural land and forest fires. In addition, with growing desertification, dust storms may become major contributors to contaminants in the air.
Air pollutions are mostly emitted by local sources but some fraction of the pollution is also transported through the atmosphere from the sources located outside, sometimes in a far distance.
Urban settings Urban pollution comes from many sources, stationary (industrial emissions) and mobile (vehicles), as well as natural ones, such as soil erosion.
Urban air pollution is caused by a mixture of pollutants including: 1. sulfur oxides (SOx), 2. nitrogen oxides (NOx), 3. carbon monoxide (CO), 4. ozone (O3) 5. organic compounds (VOCs) such as benzene, toluene, xylene and benzo(a)pyrene 6. lead is a noteworthy air contaminant in countries where it is added to gasoline, 7. particulate matter (PM).
Several of pollutants are very toxic and/or carcinogenic.
These pollutants are further transformed by processes in the atmosphere. For example, ground level ozone is a secondary pollutant produced by the interaction of sunlight with nitrogen dioxide and volatile organic compounds. Temperature and humidity are also important.
Environmental particulate air pollution is measured using several measures: - TSP – the mass of total suspended particles; - PM10 - mass of particles with an aerodynamic diameter of 10 µm. This closely corresponds to the mass fraction of inhaled particles that penetrates beyond the larynx to the airways. - PM2,5 -mass of particles with an aerodynamic diameter of 2,5 µm. The respirable fraction, which penetrates to the unciliated regions of the lung.
Particles that are less than 100 nm in diameter are commonly defined as ultrafine. Ultrafine particles are found to a large extent in urban air as both singlet and aggregated particles. Ultrafine particles are very small compared with the cellular structures and so this may be important in the apparent problems they present to the lung. Particles of diesel exhaust may be taken as an example of an ultrafine particle. They are largely insoluble because of the particulate carbon core, commonly the size of singlet diesel particles is 10–20 nm. However, they tend to group into aggregates with sulphates, metals, and hydrocarbons.
In many cities, urban air pollution is magnified by heavily polluting industrial complexes, which, although initially located and built outside the city, following urban developments are now located within the city or close to its periphery. The stationary sources that contribute most to the volume of air pollution emissions are: 1. the energy and heat generation sector, 2. the mining industry, 3. the metals industry, and 4. the chemicals industry, including refineries. Among them, the biggest polluters are power generation stations.
At the same time, both the absolute and relative amounts of pollution emitted by mobile sources are becoming more important, as traffic increases and emissions from industry decreases.
For example, here in Russia the mobile sources are rapidly growing in number and so are their emissions. The vehicle fleet, both public and private, is ageing on average. It is still using poor quality motor fuels. Poor maintenance of old vehicles, the lack of effective traffic management and the decline of public transport in most urban areas complete the picture. As a result of down-sizing of stationary sources and drastic decrease in public transport volume the share of mobile sources in total national emissions of nitrogen oxides, VOCs and carbon monoxide has been systematically increasing. In some cities transport is responsible for up to 75% of total emission of selected pollutants, and is solely responsible for air toxins like benzo(a)pyrene and soot. Health effects Health impacts of exposure to air pollutants present in urban atmosphere are well recognized. Studies conducted in many parts of the world in the recent decades have demonstrated a wide range of health effects associated with the pollution in concentrations commonly observed in the cities.
Mortality For Western countries, it is estimated that tens of thousand of premature deaths annually are associated with the pollution. Studies have found increased risk of cardiopulmonary and noncancer respiratory deaths with exposure to ambient particulate matter, ozone, and nitrogen oxides.
Morbidity Numerous epidemiologic time-series studies have shown generally consistent associations of outdoor (ambient) air pollution with cardiovascular hospital admissions.
PM and Health Several studies on short-term effects have found that ambient PM increases cardiac arrhythmia, decreases heart rate variability, increases the inflammatory response measured by C-reactive protein (CRP), and increases blood viscosity as well as other blood markers (e.g., hemoglobin, fibrinogen, platelet counts, white cell counts). These observed effects would provide a mechanism by which chronic exposure to ambient air pollution is associated with risk of coronary heart disease (CHD).
Estimated effects of air pollution on daily mortality
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
Последнее изменение этой страницы: 2017-02-07; просмотров: 274; Нарушение авторского права страницы; Мы поможем в написании вашей работы! infopedia.su Все материалы представленные на сайте исключительно с целью ознакомления читателями и не преследуют коммерческих целей или нарушение авторских прав. Обратная связь - 3.143.9.115 (0.301 с.) |