Мы поможем в написании ваших работ!
ЗНАЕТЕ ЛИ ВЫ?
|
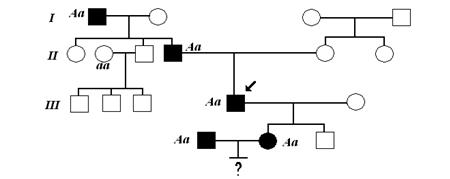
Unilateral condylar fractures
Содержание книги
- Клиника, диагностика, лечение.
- Характеристика термических ожогов
- Лечение. Лечение больных с ожогами, в том числе лица, включает комплекс общих и местных воздействий на организм пострадавшего и пораженную область.
- Тема № 21. Уход и питание потерпевших с травмой челюстно-лицевой области. Лфк и физиотерапия в комплексном лечении потерпевших с повреждениями челюстно-лицевой области.
- Режим питания больных с челюстно-лицевой травмой
- Медицинская документация, которая ведется стоматологом на мпп в военное время и порядок её заполнения
- Внештатные постоянно-действующие военно-врачебные
- Определение временной потери трудоспособности при заболеваниях челюстно-лицевой области
- Организация экспертизы временной нетрудоспособности граждан
- Tasks for individual work during preparation to lesson.
- History of the injury and description of the patient's symptoms
- Basic therms, parametrs, characterics whith are nessesery during preparation to lesson.
- Basic therms, parametrs, characterics whith are nessesery during preparation to lesson.
- А. Questions for self - checking :
- А . Questions for self-checking:
- Basic therms, parametrs, characterics whith are nessesery during preparation to lesson.
- А . Questions for self-checking:
- Basic therms, parametrs, characterics whith are nessesery during preparation to lesson.
- А . Questions for self-checking:
- Tasks for individual work during preparation to lesson.
- Injuries to the primary dentition
- Injuries to the alveolar bone
- D. Educational tasks of 3th levels (atypical tasks):
- Tasks for individual work during preparation to lesson.
- Basic knowledge, abilities, skills, which are necessary for study themes ( intradisciplinary integration) .
- Unilateral condylar fractures
- Fractures of the parasymphysis and symphysis
- Signs and symptoms common to Le Fort II and III fractures
- Signs and symptoms peculiar to Le Fort III fractures
- Unilateral Le Fort I, II and Ill-type fractures
- Theme 11. Damage of zygomatic bones and nasal bones in peace-time. Classification, frequency, clinic, diagnostics, treatment. Achievements of native scientists, employees of department.
- Tasks for individual work during preparation to lesson.
- Theme № 13. Seminar. Damages of soft tissues of maxillofacial area and bones of the facial skeleton to a peace time and in extreme conditions.
- Base knowledge, skills, the skills necessary for studying of the theme (interdisciplinary integration).
- Contused wound (Vulnus consutum)
- Characteristics of wound process
- Primary surgical treatment of a wound
- Materials for self-checking:
- Basic therms, parametrs, characterics whith are nessesery during preparation to lesson.
- Basic knowledge, abilities, skills, which are necessary for study themes (intradisciplinary integration)
- Fractures of the tooth-bearing section of the mandible
- Relative indications for removal of a tooth from the fracture line:
- Intermaxillary fixation (IMF)
- Materials for self-checking:
- Theme № 16. osteosynthesis, methods of fixing of fragments of bones of the facial skull. Achievements of native scientists, colleagues of chair.
- Osteosynthesis without intermaxillary fixation
- Non-compression small plates
- Reconstruction of the facial skeleton
- Base knowledge, skills, the skills necessary for studying of the theme (interdisciplinary integration).
- Involvement of the brain and cranial nerves
Inspection
Any movement of the lower jaw is likely to be restricted and painful. There is often swelling over the temporo-mandibular joint area and there may be haemorrhage from the ear on that side. Bleeding from the ear results from laceration of the anterior wall of the external auditory meatus, caused by violent movement of the condylar head against the skin in this region. In the normal subject the close relationship of the condyle to the skin of the external auditory meatus can be appreciated if the little finger is placed within the external ear and the jaw moved.
It is important to distinguish bleeding originating in the external auditory canal from the more serious middle ear haemorrhage. The latter signifies a fracture of the petrous temporal bone and may be accompanied by cerebrospinal otorrhoea. In all cases of suspected condylar fracture the ear should be examined carefully with an otoscope. The appearance may be extremely confusing even to an experienced maxillofacial surgeon, and there should be no hesitation in asking the opinion of an otologist in these circumstances.
The haematoma surrounding a fractured condyle may track downwards and backwards below the external auditory canal. This gives rise to ecchymosis of the skin just below the mastoid process on the same side. This particular physical sign also occurs with fractures of the base of the skull, when it is known as «Battle's sign». It is vital not to confuse the aetiology when an ecchymosis at this site is discovered
On the very rare occasion when the condylar head is impacted through the glenoid fossa, the mandible will be locked and middle ear bleeding may present externally.
If the condylar head is dislocated medially and all oedema has subsided due to passage of time, it may be possible to observe a characteristic hollow over the region of the condylar head, but in the immediate post-traumatic phase this physical sign is obscured by oedema.
Palpation
In the recently injured patient there is invariably tenderness over the condylar area. When post-traumatic oedema is present it is difficult to palpate the condylar head and what is believed to be the condylar head may, in fact, be that portion of the condylar neck continuous with the lower portion of the ramus. It may be possible to determine whether the condylar head is displaced from the glenoid fossa by palpation within the external auditory meatus. Standing in front of the patient both little fingers can be hooked into each external auditory meatus and the position and movement of each condylar head compared.
Intra-ora l.
Displacement of the condyle from the fossa or over-riding of the fractured condylar neck shortens the ramus on that side and produces gagging of the occlusion on the ipsilateral molar teeth. The mandible deviates on opening towards the side of the fracture and there is usually painful limitation of protrusion and lateral excursion to the opposite side.
Bilateral condylar fractures
The signs and symptoms already mentioned for the unilateral fracture may be present on both sides. Overall mandibular movement is usually more restricted than is the case with a unilateral fracture.
Intra-orally
It only requires one condyle to be displaced with shortening of the ramus to lead to premature contact of the posterior teeth on the side of injury. Accordingly derangement of the occlusion is more usual with bilateral than with unilateral condylar fractures. Intracapsular fractures produce little if any shortening and the occlusion is often found to be normal. If both fractures have resulted in displacement of the condyles from the glenoid fossa or overriding of the fractured bone ends, an anterior open bite is found to be present. In all cases of bilateral fracture there is pain and limitation of opening with restricted protrusion and lateral excursions.
Bilateral condylar fractures are frequently associated with fracture of the symphysis or parasymphysis and these areas should always be carefully examined.
|